




The superbug Clostridioides difficile, or C. diff, can cause dangerous intestinal infections. There are limited treatment options, and patients often face repeated infections, which can be fatal. Now, a new study shows that this dangerous bacterium can quickly develop resistance to antibiotics, although this resistance comes at a cost to the superbug itself. Researchers have identified two different mechanisms of drug resistance in C. difficile.
Toxins produced by Clostridioides difficile strains in the gastrointestinal tract cause pseudomembranous colitis, usually following antibiotic use. Symptoms include diarrhea, sometimes bloody, rarely progressing to toxic megacolon, colonic perforation, sepsis, and acute abdomen.
The study authors say the findings highlight the need for careful monitoring of bacterial resistance to antibiotics, particularly in hospitals.
In most people, the good bacteria that live in the intestines protect it from infection. When these bacteria are killed — for example, by treating an unrelated infection with antibiotics — the colon becomes vulnerable, and that’s when C. difficile attacks. People who take or have recently taken antibiotics are 10 times more likely to become infected with C. difficile than those who haven’t. Other risk factors include being in a hospital or nursing home, having a weakened immune system, or being very young or very old.

Pseudomembranous colitis
Unfortunately, only three antibiotics are available to treat C. difficile infections. Vancomycin is the drug of choice for most patients, but about a third of patients experience a return of the infection within a month of finishing treatment. One possible reason for this, the study authors suggested, is that C. difficile evolves to resist vancomycin.
“We don’t know if resistant strains are circulating and causing human infections because hospital labs don’t test for vancomycin resistance,” study author Jessica Buddle, a doctoral student at the University of Sheffield in the U.K., told Live Science. “There have only been a few reports of resistance worldwide. However, given the lack of testing, this is likely not the whole story.”
To find out whether bacteria could develop resistance to vancomycin, the researchers genetically modified two populations of C. difficile: one with a normal mutation rate and one that evolved more quickly. For the new study, published Aug. 15 in the journal PLOS Biology, they grew five strains of each population in the presence of increasing concentrations of vancomycin.
Within four days, nine of the 10 strains had developed resistance to vancomycin; by the end of the 60-day experiment, all 10 strains were able to grow with 32 times the amount of vancomycin typically used to treat C. difficile infections.
Although the bacteria used several different genetic mutations to evade vancomycin, all the resistant strains had one thing in common: They couldn’t grow as quickly as C. difficile that hadn’t developed resistance to vancomycin. In addition, several strains were smaller or had difficulty producing the spores the bacteria uses to survive and spread in the environment.
Clostridium Difficile
“In this study, the resistance that C. difficile develops to vancomycin is self-defeating because it also appears to reduce the bacteria’s ability to survive in other ways,” Dr. Paul Feuerstadt, a gastroenterologist and clinical professor of medicine at the Yale School of Medicine in Connecticut, told Live Science in an email. That may be why high-level vancomycin resistance is not as common in C. difficile as it is in some other bacteria, he added.
However, understanding and preventing antibiotic resistance is critical to ensuring that C. difficile infections are curable.
Knowing how C. difficile resists antibiotics allows scientists to develop new treatments that are harder to resist, said Feuerstadt, who was not involved in the study. Clearing infections quickly and effectively not only prevents the bacteria from becoming resistant, it also means they can’t survive long enough to develop faster growth or better transmission.
“Identifying the resistance problem will mean we make the right choices in future treatment guidelines,” Buddle said. “If we use the right drug to treat an infection and take the full course as prescribed, we increase the chances of successfully treating the infection and reduce the risk of resistance. We need to treat antibiotics as a precious resource – and everyone has a role to play.”
Meanwhile, antibiotic-resistant bacteria could cause the deaths of more than 39 million people over the next 25 years, according to a study by an international team of scientists published in an article in the medical journal The Lancet.
“We estimate that by 2050, there will be 1.91 million AMR-associated and 8.22 million AMR-attributable deaths worldwide each year. Taken together, from 2025 to 2050, our reference scenario projects 39.1 million AMR-associated and 169 million AMR-attributable deaths,” the article says.
The scientists predict the highest number of deaths in South and East Asia, as well as in Oceania and sub-Saharan Africa.
Bacterial pathogens that are resistant to antibiotics are called resistant or superbugs. According to WHO statistics, infections associated with them are the third leading cause of death in the world after heart disease and stroke. In 2019, they killed 4.95 million people. Of greatest concern is Staphylococcus aureus, which is resistant to methicillin and other antibiotics.
Clostridioides difficile (Latin: Clostridioides difficile, traditional name Clostridium difficile, synonym Peptoclostridium difficile) is a species of ubiquitous bacteria. Infections caused by Clostridioides difficile are a leading cause of diarrhea and mortality in hospitals.
Until recently, the species Clostridium difficile belonged to the genus Clostridium, which is part of the family Clostridiaceae, order Clostridiales, class Clostridia and was called Clostridium difficile. Recently, the place of this species in the taxonomy of bacteria has changed several times, it was reclassified to the genus Peptoclostridium, given the name Peptoclostridium difficile, and in 2016 it was transferred to the newly organized genus Clostridioides, which was included in the family Peptostreptococcaceae, the same order Clostridiales and class Clostridia, phylum Firmicutes, <group without rank> Terrabacteria group, kingdom Bacteria and therefore began to be called Clostridioides difficile (acceptable equivalent name Clostridium difficile.
Clostridium difficile infection
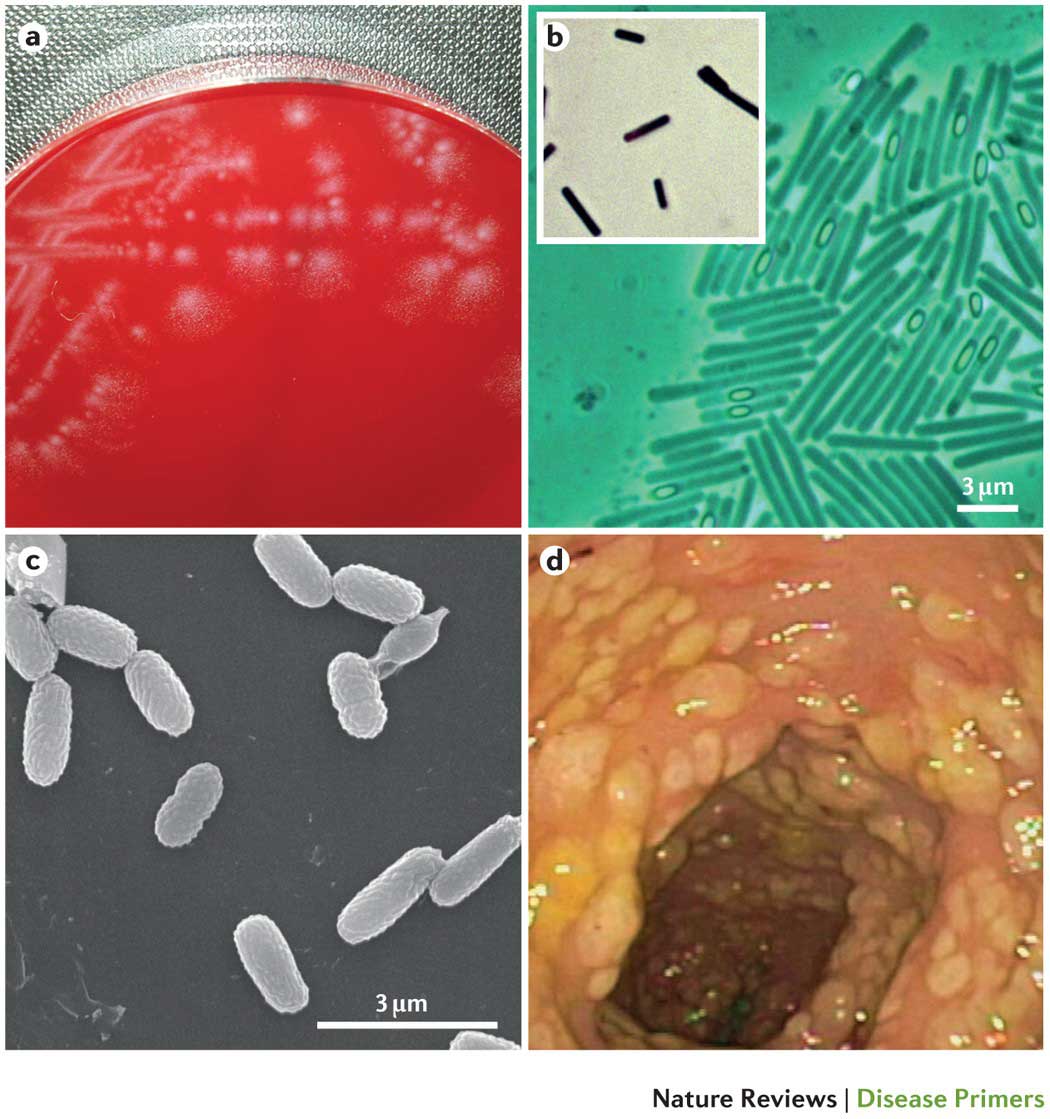
Clostridioides difficile are gram-positive, spore-forming, strictly anaerobic bacteria that are large, elongated rods with a bulge in the middle. Clostridioides difficile can survive in the environment for a long time. Its spores are resistant to heat treatment. Clostridioides difficile is naturally resistant to most antibiotics.
Toxigenic strains of Clostridioides difficile produce several pathogenic factors. The most studied of them are:
– toxin A (enterotoxin)
– toxin B (cytotoxin)
– a protein that inhibits intestinal peristalsis
Clostridium difficile is part of the normal microflora of the gastrointestinal tract (mainly inhabiting the large intestine, but can be found in the small intestine and oral cavity) and female genital tract and, sometimes, skin. Clostridium difficile is present in the intestines of approximately half of newborns and in 3–15% of healthy children over 2 years of age and adults. The amount of Clostridium difficile in the normal microflora of the intestines of a healthy adult does not exceed 0.01–0.001%. However, when taking antibiotics, the latter figure can increase to 15–40%.
Antibiotic-associated diarrhea (AAD) is one of the complications occurring in 5–25% of patients taking antibiotics. Clostridium difficile is not the only cause of AAD, although it is quite common (approximately one third of cases). Salmonella spp., Clostridium perfringens type A, Staphylococcus aureus, Klebsiella oxytoca, Candida fungi and other microorganisms can also cause AAD. AAD is one of the most common hospital-acquired infections. In the United States alone, up to 1 million cases of AAD are registered annually. Despite the significant carriage of Clostridium difficile, infants almost never suffer from AAD caused by Clostridium difficile.
The occurrence of AAD is due to the fact that antibiotics suppress not only pathogenic, but also normal intestinal microflora, which under normal conditions does not allow pathogenic and opportunistic microorganisms to multiply. As a result of the effect of antibiotics on normal microflora, the number of drug-resistant pathogenic and opportunistic microbes (including Clostridium difficile) in the human body can increase significantly.
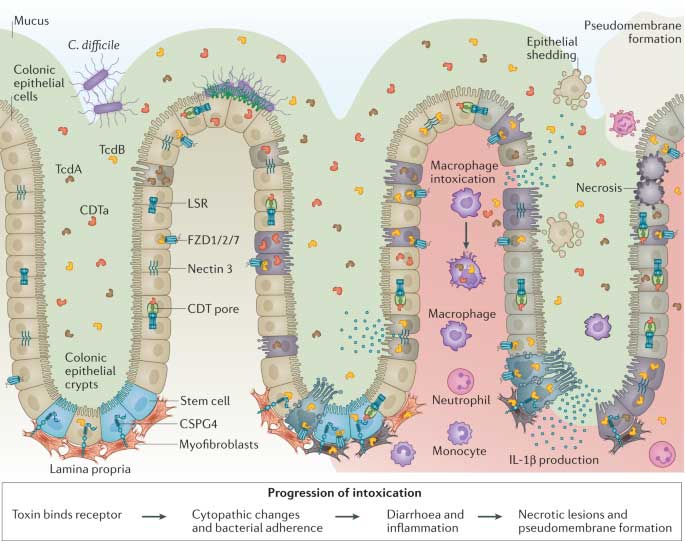
Clostridioides difficile toxins: mechanisms of action and antitoxin therapeutics
Almost any antimicrobial agent can cause AAD, but the incidence of the disease depends significantly on the type of antibiotic (although it does not depend on the dose). Most often, AAD is caused by taking clindamycin, cephalosporins, and ampicillin.
Symptoms of AAD range from mild diarrhea to severe enterocolitis called pseudomembranous colitis. Pseudomembranous colitis is caused in the vast majority of cases by Clostridium difficile infection.
The main risk factor for severe forms of AAD caused by Clostridium difficile is antibiotic therapy. Even a single dose of a broad-spectrum antibiotic, regardless of the dose and route of administration, can lead to the development of AAD and pseudomembranous colitis. A long hospital stay, especially in the same ward with Clostridium difficile carriers, is also a risk factor.
Pseudomembranous colitis is characterized by profuse, frequent watery diarrhea, sometimes with blood, mucus, and pus. As a rule, diarrhea is accompanied by fever, elevated to 38.5–40°C, moderate or intense abdominal pain of a cramping or constant nature. Mortality in the absence of treatment for patients with pseudomembranous colitis is 15–30%.
A characteristic feature of Clostridium difficile infection is its frequent relapses – on average 20-25%, caused by the presence of Clostridium difficile spores in the intestine or re-infection. Recovery or improvement usually occurs after treatment, but on the 2nd-28th day (on average after 3-7 days) a relapse occurs, identical to the initial episode.
Diagnosis and treatment of AAD caused by Clostridium (Clostridioides) difficile
The main damaging factors of the human body in diseases caused by Clostridium difficile are toxins A and B. Not all strains of Clostridium difficile produce these toxins. In order to detect infection with toxigenic strains of Clostridium difficile, a stool test is performed for the presence of toxins A and B or a stool test – culture for Clostridium difficile. Normally, the test results should be negative.
If AAD is detected, the antibiotic that caused the disease must be discontinued. Treatment of severe cases of AAD and pseudomembranous colitis includes therapy with vancomycin or metronidazole, to which most strains of Clostridium difficile are sensitive. Taking antidiarrheal drugs and antispasmodics is not allowed due to the risk of developing a severe complication – toxic megacolon.
Of the probiotics, Enterol is effective, containing lyophilized yeast fungi Saccharomyces boulardi, which have a direct antimicrobial effect not only on Clostridium difficile, but also on other microorganisms that can cause AAD. To prevent the development of AAD and restore intestinal microflora after discontinuing an antibiotic (vancomycin or metronidazole), drugs containing strains of representatives of the natural microflora are used: Lactobacillus acidophilus, Lactobacillus rhamnosus, Bifidobacterium longum, Enterococcus faecium and others (Linex, Bifiform, etc.).
The World Gastroenterology Organization notes the effectiveness of the use of the Lactobacillus casei strain DN-114 001 for the treatment of Clostridium difficile-associated diarrhea, as well as for its prevention (Probiotics and prebiotics. Practical recommendations):
– Lactobacillus casei DN-114 001 in fermented milk with Lactobacillus bulgaricus and Streptococcus thermophilus 1010 CFU, 2 times a day
– Lactobacillus acidophilus + Bifidobacterium bifidum (special strains) – 2 x 1010 CFU each, 1 time per day
– Saccharomyces cerevisiae (boulardii). Age 1 year – 2 x 1010 CFU per day
– Oligofructose – 4 g, 3 times a day for 4 g.
Antibacterial agents active against Clostridium difficile: vancomycin, metronidazole, rifaximin, tetracycline, doxycycline, lincomycin. Clostridium difficile is resistant to ciprofloxacin. On October 21, 2016, the US FDA approved a new drug for the prevention of relapse of Clostridium difficile infection in patients over 18 years of age for use in the US – bezlotoxumab, trade name Zinplava. Bezlotoxumab is a monoclonal antibody designed to neutralize Clostridium difficile toxin B.

